Beyond “Too Much Sugar”: The Real Trigger
Type 2 diabetes (T2D) is often blamed on carbohydrates, but the proximate cause is chronic energy surplus, especially when calorie intake persistently outpaces expenditure while physical activity is low. Once the body exhausts its genetically limited capacity to store fat safely under the skin, it begins packing excess triglycerides deep inside the abdomen (omentum, mesentery, liver, even skeletal muscle). This state is known as visceral obesity. (Type 2 Diabetes: Causes, Symptoms, Treatments – 2025)
Visceral Fat as an Endocrine Organ
Unlike subcutaneous fat, visceral adipose tissue constantly secretes inflammatory cytokines and, crucially, ceramides. These bio-active sphingolipids are more than passive by-products; they are molecular saboteurs of insulin signaling.
What exactly are ceramides a plain-language guide
Think of a ceramide as a tiny wax plug made from fat.
- What it’s built from. Picture a short “backbone” (the amino-alcohol sphingosine) with a single fatty-acid tail snapped on. Put millions of those plugs side-by-side and you get the waterproof seal in human skin. The very word comes from Latin cera – “wax.”
- Where the plugs are made. Inside the cell’s workshop (the endoplasmic reticulum) an enzyme rivets serine to palmitoyl-CoA → the first, rough wax plug → it is polished into a finished ceramide. The more saturated fat and calories that reach the workshop, the faster the assembly line runs
Why we need a few of these plugs
- Skin waterproofing: Millions of ceramides stack between skin cells, sealing in moisture and keeping germs and allergens out your natural lotion.
- Cell-signaling rafts & nerve insulation: In cell membranes they help cluster receptors so messages fire on time, and they are raw material for the myelin that insulates nerves. In short, a normal trickle of ceramides keeps tissues watertight, messages clear, and nerves quick.
Why too many ceramides become a problem
Imagine every muscle or liver cell has a sliding garage door for glucose. Insulin presses the “open” button; wires carry the signal to the motor (the protein AKT) the door (GLUT-4) rolls up and sugar drives in. When ceramides pile up inside these organs, they act like gummy wax that
- Coats the wiring deactivates AKT, so the motor never whirs and the glucose door stays shut.
- Flicks on the fire alarm triggers NF-κB, summoning inflammatory chemicals that further jam the mechanism.
- Gums up the generators clogs mitochondria, cutting the cell’s ability to burn fuel, which leaves even more fat sloshing around to make… more ceramides.
So, in moderate amounts ceramides are indispensable sealants and messengers; in excess they become sticky saboteurs that shut the door on insulin – exactly what happens during visceral-fat overload.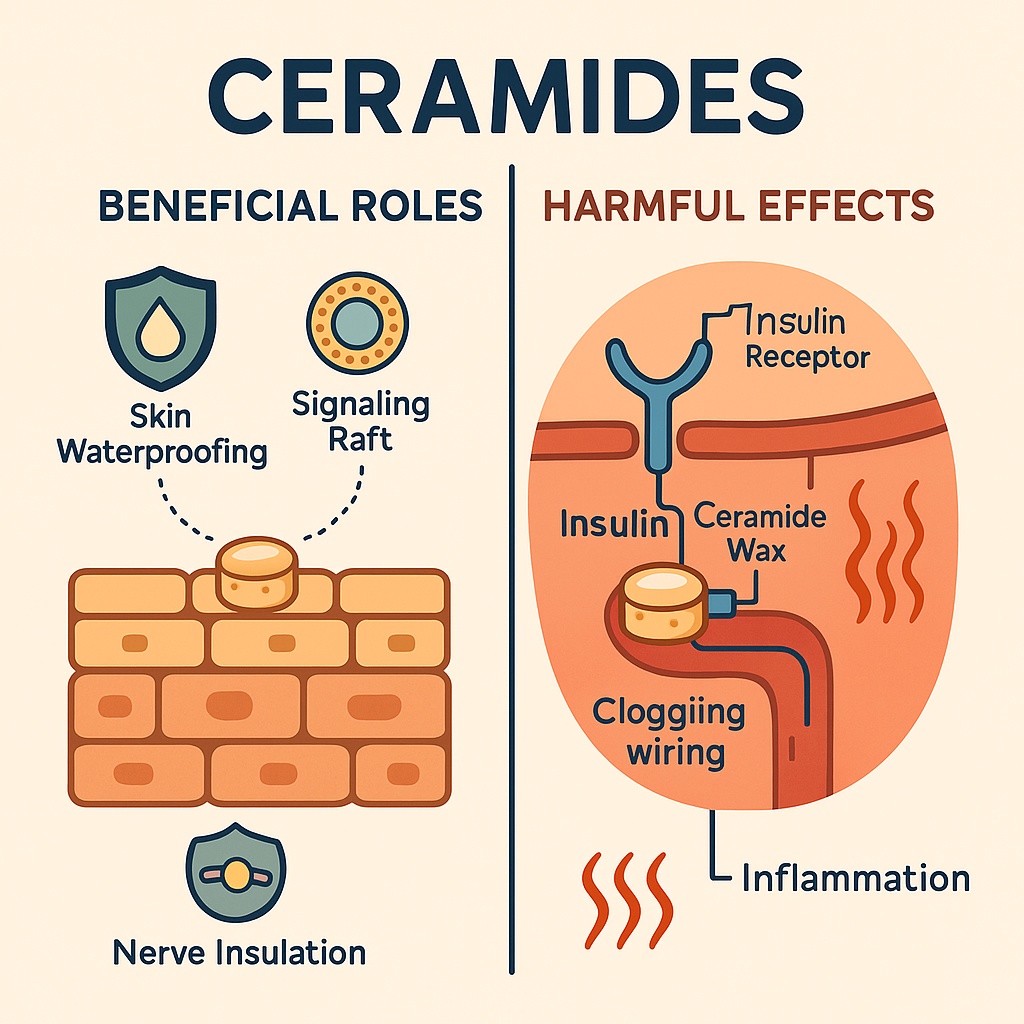
Ceramides: Blocking the Insulin Signal
Under normal circumstances, insulin binds its receptor, activates the kinase AKT, and shuttles GLUT-4 transporters to the cell membrane so that glucose can enter. Ceramides interrupt this cascade:
- Direct inhibition of AKT → GLUT-4 never reaches the surface → glucose remains in the blood.
- Activation of NF-κB → amplification of inflammatory cytokines (TNF-α, IL-6).
- Mitochondrial damage in muscle → reduced fat and glucose oxidation.
- Suppressed adiponectin → further loss of insulin sensitivity.
- β-cell stress and apoptosis → dwindling insulin production.
The result is a self-reinforcing loop: more visceral fat → more ceramides → more insulin resistance → higher blood glucose → still more fat deposition.
Clinical Proof: The DiRECT Study
Compelling evidence that breaking this loop restores metabolic health comes from the UK Diabetes Remission Clinical Trial (DiRECT). In this cluster-randomised primary-care study, people with T2D who lost 10–15 kg over 12 months achieved remission in up to 86 % of cases without drugs. Imaging showed parallel shrinkage of fat in the liver and pancreas, with corresponding drops in ceramide production and a rebound in insulin sensitivity. Read the Lancet paper →
Translating Mechanism into Action
Because ceramide oversupply is driven by energy excess, reversing T2D hinges on creating a sustained energy deficit and reducing visceral fat. Evidence-based levers include:
| Lever | How It Helps the Mechanism |
|---|---|
| Caloric restriction / meal-replacement programs | Lowers hepatic & pancreatic fat → fewer ceramides → reinstates AKT signaling |
| Progressive resistance & aerobic training | Expands glucose “sink” in muscle; boosts mitochondrial biogenesis; counters NF-κB activation |
| Whole-food, high-fiber diet | Naturally lowers caloric density, blunts post-prandial lipid spikes that feed ceramide synthesis |
| Adequate sleep & stress management | Reduces cortisol-driven lipolysis and inflammatory tone, indirectly limiting ceramide flux |
| GLP-1 receptor agonists (e.g., Rybelsus ® / oral semaglutide) | Curb appetite, slow gastric emptying and raise post-meal satiety → sustained energy deficit and clinically significant weight and visceral-fat loss; GLP-1 signaling also up-regulates ceramidase activity, directly lowering harmful ceramide species and easing the blockade on insulin pathways. How it works, Rybelsus Cost |
Important: Remission is conditional. If calorie surplus returns and visceral fat creeps back, ceramide production resumes and the disease pathway restarts even years later.
Note: GLP-1 RAs are most effective when layered on top of lifestyle changes, not as stand-alone fixes; they help create and sustain the energy deficit that ultimately shrinks visceral fat and its ceramide output. (The Future of Oral GLP-1)
Key Takeaways
- Visceral fat is an endocrine tissue whose ceramide output short-circuits insulin action.
- The root driver is long-term energy surplus, not carbohydrates per se.
- Weight loss of ~10 kg, preferably via structured, lifestyle-based programs can switch off ceramide production, restore insulin sensitivity, and put T2D into remission, as demonstrated in the DiRECT trial.
- Long-term success depends on maintaining an energy balance that keeps visceral fat, and thus ceramides, at bay.
Armed with an understanding of this mechanism, patients and clinicians can move beyond symptom-focused glucose lowering and target the true upstream cause: too much energy stored in the wrong place.